<Insert Unit Code and Title>
<Unit Code> – Assessment Task # Page 3 of 15
Assessment Task 1
Assessment name: Case Study: The Deteriorating Patient
Task description: For this essay you are required to select ONE case scenario related to the clinical deterioration of a patient: Option 1: Traumatic Brain Injury Option 2: Septic Shock
What you need to do: In order to undertake this 1500 word essay you will need to research the topic using current and relevant peer reviewed literature and review of:
The lecture and tutorial material associated with the relevant topic.
Your knowledge and understanding related to: 1. The physiology and pathophysiology of the primary
diagnosis and associated clinical data identified within the chosen case study;
2. The physiological assessments relevant to the features within the case study.
The assessment tasks requires you to:
1. Identify and discuss two (2) signs or symptoms of clinical deterioration associated with the presenting problem, from chosen case study. This discussion should consider the potential impact of case study data (e.g. pathology results, past medical history) on the health status of the patient in the chosen case. 2. Following on from your presented discussion associated with point one (1), develop a clinical plan of care which identifies:
One (1) priority of clinical care and;
Discuss three (3) nursing interventions that directly address the identified clinical priority. The discussion should refer to relevant clinical assessments. Measurable outcome parameters for each intervention will be discussed to justify the intervention and evaluate its efficacy. Discussion is to be supported with contemporary research.
Length: 1500 words +/-10% (word length includes in-text referencing and excludes your reference list)
Estimated time to complete task:
Approximately 30 hours
Weighting: 50%
How will I be assessed: As a percentage using a 7-point grading scale rubric
Due date: Friday September 21st submitted via Turnitin in your <Unit Code> Blackboard site by 23:59 hours. More information about Turnitin is available on the FAQs about Turnitin page.
Presentation requirements:
This assessment task must:
Be a written academic essay containing an introduction, body
<Unit Code> – Assessment Task # Page 3 of 15
Assessment Task 1
Assessment name: Case Study: The Deteriorating Patient
Task description: For this essay you are required to select ONE case scenario related to the clinical deterioration of a patient: Option 1: Traumatic Brain Injury Option 2: Septic Shock
What you need to do: In order to undertake this 1500 word essay you will need to research the topic using current and relevant peer reviewed literature and review of:
The lecture and tutorial material associated with the relevant topic.
Your knowledge and understanding related to: 1. The physiology and pathophysiology of the primary
diagnosis and associated clinical data identified within the chosen case study;
2. The physiological assessments relevant to the features within the case study.
The assessment tasks requires you to:
1. Identify and discuss two (2) signs or symptoms of clinical deterioration associated with the presenting problem, from chosen case study. This discussion should consider the potential impact of case study data (e.g. pathology results, past medical history) on the health status of the patient in the chosen case. 2. Following on from your presented discussion associated with point one (1), develop a clinical plan of care which identifies:
One (1) priority of clinical care and;
Discuss three (3) nursing interventions that directly address the identified clinical priority. The discussion should refer to relevant clinical assessments. Measurable outcome parameters for each intervention will be discussed to justify the intervention and evaluate its efficacy. Discussion is to be supported with contemporary research.
Length: 1500 words +/-10% (word length includes in-text referencing and excludes your reference list)
Estimated time to complete task:
Approximately 30 hours
Weighting: 50%
How will I be assessed: As a percentage using a 7-point grading scale rubric
Due date: Friday September 21st submitted via Turnitin in your <Unit Code> Blackboard site by 23:59 hours. More information about Turnitin is available on the FAQs about Turnitin page.
Presentation requirements:
This assessment task must:
Be a written academic essay containing an introduction, body
<Insert Unit Code and Title>
<Unit Code> – Assessment Task # Page 4 of 15
and conclusion, addressing the task. Use QUT APA referencing for citing academic literature (see
http://www.citewrite.qut.edu.au/). Assignment cover sheet must be included as the first page of
your document. Be submitted in electronic form via Turitin. A minimum of 15 relevant references to be cited from valid,
contemporary journal articles or books no older than 7 years. The use of websites as references is NOT permitted. The submitted essay should NOT contain tables, figures or
appendices. The uses of dot points are NOT permitted.
Your assignment should be prepared as follows: Has a cover sheet with the assessment title, your name, student
number, tutor name and word count. Coversheet template is recommended.
Include a ‘footer’ on each page with your name, student number, unit code and page number.
3 cm margins on all sides, double-spaced text Times new roman, font size 12 APA style referencing (see http://www.citewrite.qut.edu.au/) Headings can be used to structure your assignment logically (if
applicable)
be submitted in electronic format via Turnitin.
Learning outcomes assessed:
1. Consolidate knowledge of key NMBA Registered Nurse Standards for Practice, National Safety and Quality Health Services Standards, and National Health Priorities to enable effective decision planning and action in a range of complex clinical situations across the lifespan.
2. Apply knowledge of anatomy, physiology and pathophysiology to
support evidence based decision making associated with planning and action.
3. Demonstrate structured decision making and clinical reasoning to review a range of health situations, synthesise evidence and data, determine priorities and formulate plans of care and interventions in line with timeframes and agreed goals.
What you need to submit:
One word document that contains the following items: 1. Assignment Cover Sheet & responses to Question 1 & 2 2. Must be submitted in electronic form via Turitin by the assigned
date.
Resources needed to complete task:
Case studies and clinical documents available within this document.
<Unit Code> – Assessment Task # Page 4 of 15
and conclusion, addressing the task. Use QUT APA referencing for citing academic literature (see
http://www.citewrite.qut.edu.au/). Assignment cover sheet must be included as the first page of
your document. Be submitted in electronic form via Turitin. A minimum of 15 relevant references to be cited from valid,
contemporary journal articles or books no older than 7 years. The use of websites as references is NOT permitted. The submitted essay should NOT contain tables, figures or
appendices. The uses of dot points are NOT permitted.
Your assignment should be prepared as follows: Has a cover sheet with the assessment title, your name, student
number, tutor name and word count. Coversheet template is recommended.
Include a ‘footer’ on each page with your name, student number, unit code and page number.
3 cm margins on all sides, double-spaced text Times new roman, font size 12 APA style referencing (see http://www.citewrite.qut.edu.au/) Headings can be used to structure your assignment logically (if
applicable)
be submitted in electronic format via Turnitin.
Learning outcomes assessed:
1. Consolidate knowledge of key NMBA Registered Nurse Standards for Practice, National Safety and Quality Health Services Standards, and National Health Priorities to enable effective decision planning and action in a range of complex clinical situations across the lifespan.
2. Apply knowledge of anatomy, physiology and pathophysiology to
support evidence based decision making associated with planning and action.
3. Demonstrate structured decision making and clinical reasoning to review a range of health situations, synthesise evidence and data, determine priorities and formulate plans of care and interventions in line with timeframes and agreed goals.
What you need to submit:
One word document that contains the following items: 1. Assignment Cover Sheet & responses to Question 1 & 2 2. Must be submitted in electronic form via Turitin by the assigned
date.
Resources needed to complete task:
Case studies and clinical documents available within this document.
<Insert Unit Code and Title>
<Unit Code> – Assessment Task # Page 5 of 15
Documents such as additional readings available on your blackboard site.
Access to the prescribed texts for this unit as outlined in the unit details.
QUT Cite|Write APA guide. Turnitin Tip Sheets.
Academic Integrity The School of Nursing takes academic integrity very seriously. All work submitted must be your own work and work not previously submitted for other study. The work of others needs to be correctly acknowledged and referenced according to the APA guidelines. There are serious consequences that will be imposed should you be found to breach academic integrity. Make sure you are familiar with the MOPP C/5.3 Academic Integrity and view the Academic Integrity video and explore the Academic Case Studies available on your Blackboard site. Maintaining academic integrity is your responsibility. If in doubt, check it carefully.
Assignment Hints This assignment requires you to critically consider the signs and symptoms associated with clinical deterioration in relation to the patient’s primary clinical diagnosis, with consideration to:
The change in health status associated with the primary clinical diagnosis; How the patients clinical history may impact on assessment data and core
interventions; The identified clinical priority which should clearly emerge from your
discussion of the primary health alteration. The application of clinical data and research to identify three (3) core
interventions and assessments that address the stated clinical priority. Evaluation data supported by research to effectively determine success of
the intervention. The SMART goals format may be of assistance in guiding you in structuring this.
Demonstration of your clinical reasoning for your selected case study. Demonstrating your understanding and application of evidence based care
i.e. the research you have to support your discussion and ideas regarding clinical interventions and assessment outcomes.
Format example: The introduction to your paper should provide the reader with background
regarding the primary pathophysiological concepts being discussed, a brief overview of the case study (summation of the primary points), the objective of the paper (what you intend to address), and the rationale for the paper (why is it important to apply and understand the content).
<Unit Code> – Assessment Task # Page 5 of 15
Documents such as additional readings available on your blackboard site.
Access to the prescribed texts for this unit as outlined in the unit details.
QUT Cite|Write APA guide. Turnitin Tip Sheets.
Academic Integrity The School of Nursing takes academic integrity very seriously. All work submitted must be your own work and work not previously submitted for other study. The work of others needs to be correctly acknowledged and referenced according to the APA guidelines. There are serious consequences that will be imposed should you be found to breach academic integrity. Make sure you are familiar with the MOPP C/5.3 Academic Integrity and view the Academic Integrity video and explore the Academic Case Studies available on your Blackboard site. Maintaining academic integrity is your responsibility. If in doubt, check it carefully.
Assignment Hints This assignment requires you to critically consider the signs and symptoms associated with clinical deterioration in relation to the patient’s primary clinical diagnosis, with consideration to:
The change in health status associated with the primary clinical diagnosis; How the patients clinical history may impact on assessment data and core
interventions; The identified clinical priority which should clearly emerge from your
discussion of the primary health alteration. The application of clinical data and research to identify three (3) core
interventions and assessments that address the stated clinical priority. Evaluation data supported by research to effectively determine success of
the intervention. The SMART goals format may be of assistance in guiding you in structuring this.
Demonstration of your clinical reasoning for your selected case study. Demonstrating your understanding and application of evidence based care
i.e. the research you have to support your discussion and ideas regarding clinical interventions and assessment outcomes.
Format example: The introduction to your paper should provide the reader with background
regarding the primary pathophysiological concepts being discussed, a brief overview of the case study (summation of the primary points), the objective of the paper (what you intend to address), and the rationale for the paper (why is it important to apply and understand the content).
<Insert Unit Code and Title>
<Unit Code> – Assessment Task # Page 6 of 15
The body should include: o Discuss the physiology of the health alteration and how the signs and
symptoms you have identified reflect these changes (you may wish to consider the clinical data provided to support your discussion of ideas e.g. blood results, medical imaging and/or past medical history).
o Research you have undertaken is discussed in relation to the change in the health status of your patient, and the one (1) priority of clinical care.
o A discussion of research relevant to nursing interventions that address the clinical priority that you have identified. What can be implemented that would help address the priority of care, and why such interventions are likely to be helpful based on your research. Remember this should address key considerations for deteriorating patient, therefore nursing interventions such pressure area care may not be a major clinical priority in this context.
The research you have undertaken should assist you in identifying and discussing the key assessment parameters: e.g. what are the current research recommendations, how will you evaluate the impact of an intervention on the patient (this should be measurable e.g. oxygen saturations are greater than 95% and a justification for why 95% is the chosen target)
Conclusion: The conclusion should bring together the main objective of the paper (which you outlined in the introduction), provide a summation of the key points that you discussed (do not introduce need content into the conclusion), and provide a concluding comment regarding the clinical application of the concepts.
This unit has three main texts assigned to it, which should form the basis of your initial research and conceptual development relating to the assessment concepts, these are:
<Unit Code> – Assessment Task # Page 6 of 15
The body should include: o Discuss the physiology of the health alteration and how the signs and
symptoms you have identified reflect these changes (you may wish to consider the clinical data provided to support your discussion of ideas e.g. blood results, medical imaging and/or past medical history).
o Research you have undertaken is discussed in relation to the change in the health status of your patient, and the one (1) priority of clinical care.
o A discussion of research relevant to nursing interventions that address the clinical priority that you have identified. What can be implemented that would help address the priority of care, and why such interventions are likely to be helpful based on your research. Remember this should address key considerations for deteriorating patient, therefore nursing interventions such pressure area care may not be a major clinical priority in this context.
The research you have undertaken should assist you in identifying and discussing the key assessment parameters: e.g. what are the current research recommendations, how will you evaluate the impact of an intervention on the patient (this should be measurable e.g. oxygen saturations are greater than 95% and a justification for why 95% is the chosen target)
Conclusion: The conclusion should bring together the main objective of the paper (which you outlined in the introduction), provide a summation of the key points that you discussed (do not introduce need content into the conclusion), and provide a concluding comment regarding the clinical application of the concepts.
This unit has three main texts assigned to it, which should form the basis of your initial research and conceptual development relating to the assessment concepts, these are:
<Insert Unit Code and Title>
<Unit Code> – Assessment Task # Page 7 of 15
Case Option 1: Traumatic Brain Injury
James “Jimmy” Parsons is a 26 year old flight engineer who was admitted post- operatively to the High Dependency Unit approximately 46 hours ago. He was out with friends on Saturday night when he was involved in an altercation out the front of a bar with another group of males who had been making lude remarks about female acquaintances of Mr Parsons. During this altercation, it is alleged that one of the individuals punched Mr Parsons in the face, and as a result he lost consciousness, fell, and hit the back of his head on the pavement.
On arrival to the Emergency Department he underwent an urgent CT brain scan which revealed a sub-dural hemorrhage with 1cm mid-line shift and petechial hemorrhages, which was drained intra-operatively. A Codman’s intracranial pressure monitoring device was placed in order to monitor ICP levels post operatively. Mr Parson’s blood alcohol levels were noted to be elevated on assessment at the ED and his blood toxicology screen was negative for illicit substances. Over the immediate post-operative period he has been deemed to be stable and he has been extubated approximately 6 hours ago and is currently on Hiflow Nasal Prongs (HFNP).
Past medical History Type 1 Diabetes, smoker (7-10 cigarettes per day), social drinker (6-10 beers on weekends), wisdom teeth removal x 4 (2010).
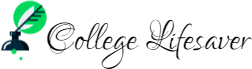
On assessment: He is lying supine (head of bed elevated 30%), Codman’s ICP monitoring insitu, GCS 10/15 (E3, V3, M4), Pupils equal and reactive to light and accommodating. There is visual evidence of raccoon eyes (see below image) and battle sign (right sided) (refer to below image).
<Unit Code> – Assessment Task # Page 7 of 15
Case Option 1: Traumatic Brain Injury
James “Jimmy” Parsons is a 26 year old flight engineer who was admitted post- operatively to the High Dependency Unit approximately 46 hours ago. He was out with friends on Saturday night when he was involved in an altercation out the front of a bar with another group of males who had been making lude remarks about female acquaintances of Mr Parsons. During this altercation, it is alleged that one of the individuals punched Mr Parsons in the face, and as a result he lost consciousness, fell, and hit the back of his head on the pavement.
On arrival to the Emergency Department he underwent an urgent CT brain scan which revealed a sub-dural hemorrhage with 1cm mid-line shift and petechial hemorrhages, which was drained intra-operatively. A Codman’s intracranial pressure monitoring device was placed in order to monitor ICP levels post operatively. Mr Parson’s blood alcohol levels were noted to be elevated on assessment at the ED and his blood toxicology screen was negative for illicit substances. Over the immediate post-operative period he has been deemed to be stable and he has been extubated approximately 6 hours ago and is currently on Hiflow Nasal Prongs (HFNP).
Past medical History Type 1 Diabetes, smoker (7-10 cigarettes per day), social drinker (6-10 beers on weekends), wisdom teeth removal x 4 (2010).
On assessment: He is lying supine (head of bed elevated 30%), Codman’s ICP monitoring insitu, GCS 10/15 (E3, V3, M4), Pupils equal and reactive to light and accommodating. There is visual evidence of raccoon eyes (see below image) and battle sign (right sided) (refer to below image).
<Insert Unit Code and Title>
<Unit Code> – Assessment Task # Page 8 of 15
Vitals
Time 08:00hrs 10:00hrs
ICP (mmHg) 10 12
Temp (°C) 36.9 37.2
Respirations (breaths/min)
18 (eupnic) 23 (increased work of breathing, associated with agitation)
Blood pressure and Mean Arterial Pressure (MAP) (mmHg)
128/92 (98) 122/68 (86)
Heart rate (beats/min)
87 96
SpO2 (Fio2) 97% (Fio2 30%, 30L high flow nasal prongs (HFNP))
96 (FiO2 30%, 30L, HFNP)
BGL 6 (Actrapid infusion at 2units/hr)
6.4 (Actrapid infusion at 2 units/hr)
At 13:00 hours Mr Parson’s becomes tachycardic with a HR 118 without a clear precipitating cause, a 12 lead ECG confirms the rhythm to be sinus tachycardia.
<Unit Code> – Assessment Task # Page 8 of 15
Vitals
Time 08:00hrs 10:00hrs
ICP (mmHg) 10 12
Temp (°C) 36.9 37.2
Respirations (breaths/min)
18 (eupnic) 23 (increased work of breathing, associated with agitation)
Blood pressure and Mean Arterial Pressure (MAP) (mmHg)
128/92 (98) 122/68 (86)
Heart rate (beats/min)
87 96
SpO2 (Fio2) 97% (Fio2 30%, 30L high flow nasal prongs (HFNP))
96 (FiO2 30%, 30L, HFNP)
BGL 6 (Actrapid infusion at 2units/hr)
6.4 (Actrapid infusion at 2 units/hr)
At 13:00 hours Mr Parson’s becomes tachycardic with a HR 118 without a clear precipitating cause, a 12 lead ECG confirms the rhythm to be sinus tachycardia.
<Insert Unit Code and Title>
<Unit Code> – Assessment Task # Page 9 of 15
At 13:10 his BP is 108/54mmHg (MAP 72), Heart rate 118-123 beats/min, temp 37.8°C (mildly diaphoretic), ICP 21mmHg, Sp02 95% (HFNP FiO2 30%, 30L), respiratory rate 11breaths/min with apneic periods (on auscultation air entry is decreased to both the left and right bases), BGL 12.1 mmol/L (Actrapid infusion at 2 units/hr), pupils equal (right side 4mm, slow reaction to light, left 4mm – brisk reaction to light). An urgent arterial blood gas is taken:
Temperature corrected result (37.8°C)
Results Reference range
pH 7.31 7.35-7.45
PaCO2 51 35-45
PaO2 88 80-100
Na 132 135-145
Cl- 105
Ca++ 1.11
Gluc 12.4
Lac 1.9 <2
Hb 89
SaO2 89
HCO3 23 22-24
Pa02/FiO2 ration 293
<Unit Code> – Assessment Task # Page 9 of 15
At 13:10 his BP is 108/54mmHg (MAP 72), Heart rate 118-123 beats/min, temp 37.8°C (mildly diaphoretic), ICP 21mmHg, Sp02 95% (HFNP FiO2 30%, 30L), respiratory rate 11breaths/min with apneic periods (on auscultation air entry is decreased to both the left and right bases), BGL 12.1 mmol/L (Actrapid infusion at 2 units/hr), pupils equal (right side 4mm, slow reaction to light, left 4mm – brisk reaction to light). An urgent arterial blood gas is taken:
Temperature corrected result (37.8°C)
Results Reference range
pH 7.31 7.35-7.45
PaCO2 51 35-45
PaO2 88 80-100
Na 132 135-145
Cl- 105
Ca++ 1.11
Gluc 12.4
Lac 1.9 <2
Hb 89
SaO2 89
HCO3 23 22-24
Pa02/FiO2 ration 293
<Insert Unit Code and Title>
<Unit Code> – Assessment Task # Page 10 of 15
Case Option 2: Shock Jedda Merindah 33 year old male of indigenous heritage who has been admitted to the Hematology/Oncology unit. Jedda was admitted post a medical emergency call for hypotension, via the oncology day unit where he was receiving chemotherapy for his Acute Myeloid Leukemia (AML).
Background: AML – induction phase chemotherapy treatment
Patient reports nil temperatures – self monitors at home
Routine blood cultures taken from Hickman’s line 1 week ago – nil growth to date.
Past Medical History Acute Rheumatic Fever as a child – previous echocardiogram reveals no structural abnormalities, mild dilation of the left ventricle, normal ejection fraction.
Depression – Citalopram 10mg daily
Previous suicide attempt (2003) – drug overdose
Hypercholesterolemia – Atorvastatin 40mg
On assessment: Neuro: GCS 15/ 15, pupils equal and reactive to light, appears anxious and restless.
Cardiovascular: HR 118 beats/min- ECG reveals atrial fibrillation, non -invasive blood pressure 92/65mmHg, 250ml NaCl 0.9% fluid challenge given in ED, Febrile (38.8°C), diaphoretic, capillary refill time (CRT) < 3 sec., cool peripheries, Hickman’s line in situ, central venous catheter line inserted by ED senior registrar.
Respiratory: Decreased air entry to left and right bases, non-productive cough, tachypneoic 28 breaths per minute, using accessory muscles, Fi02 44% via Hudson mask, SpO2 >95%.
<Unit Code> – Assessment Task # Page 10 of 15
Case Option 2: Shock Jedda Merindah 33 year old male of indigenous heritage who has been admitted to the Hematology/Oncology unit. Jedda was admitted post a medical emergency call for hypotension, via the oncology day unit where he was receiving chemotherapy for his Acute Myeloid Leukemia (AML).
Background: AML – induction phase chemotherapy treatment
Patient reports nil temperatures – self monitors at home
Routine blood cultures taken from Hickman’s line 1 week ago – nil growth to date.
Past Medical History Acute Rheumatic Fever as a child – previous echocardiogram reveals no structural abnormalities, mild dilation of the left ventricle, normal ejection fraction.
Depression – Citalopram 10mg daily
Previous suicide attempt (2003) – drug overdose
Hypercholesterolemia – Atorvastatin 40mg
On assessment: Neuro: GCS 15/ 15, pupils equal and reactive to light, appears anxious and restless.
Cardiovascular: HR 118 beats/min- ECG reveals atrial fibrillation, non -invasive blood pressure 92/65mmHg, 250ml NaCl 0.9% fluid challenge given in ED, Febrile (38.8°C), diaphoretic, capillary refill time (CRT) < 3 sec., cool peripheries, Hickman’s line in situ, central venous catheter line inserted by ED senior registrar.
Respiratory: Decreased air entry to left and right bases, non-productive cough, tachypneoic 28 breaths per minute, using accessory muscles, Fi02 44% via Hudson mask, SpO2 >95%.
<Insert Unit Code and Title>
<Unit Code> – Assessment Task # Page 11 of 15
GIT: nil reports of vomiting, decreased nutritional intake secondary to mouth ulcers, some loose bowel actions over last 2/7 days, nil malena, abdomen lax and non- tender, BGL 9.6mmol.
Renal: Decrease urinary output, patient reports dark in colour, IDC insertion pending.
Blood pathology results:
Results Reference ranges
Hb 89 130-180 g/L
White cell count 3.4 4-11 (x10*9/L)
Platelets 114 150-300 (x10*9/L)
Sodium 140 135-145 mmol/L
Potassium 4.7 3.5-5 mmol/L
Creatinine 138 60-120 µmol/L
Urea 11.2 3.6-9.3 µmol/L
Albumin 31 35-52 g/L
APTT 47 25-35 sec.
INR 2.4 0.8-1.2 units/kg
<Unit Code> – Assessment Task # Page 11 of 15
GIT: nil reports of vomiting, decreased nutritional intake secondary to mouth ulcers, some loose bowel actions over last 2/7 days, nil malena, abdomen lax and non- tender, BGL 9.6mmol.
Renal: Decrease urinary output, patient reports dark in colour, IDC insertion pending.
Blood pathology results:
Results Reference ranges
Hb 89 130-180 g/L
White cell count 3.4 4-11 (x10*9/L)
Platelets 114 150-300 (x10*9/L)
Sodium 140 135-145 mmol/L
Potassium 4.7 3.5-5 mmol/L
Creatinine 138 60-120 µmol/L
Urea 11.2 3.6-9.3 µmol/L
Albumin 31 35-52 g/L
APTT 47 25-35 sec.
INR 2.4 0.8-1.2 units/kg
<Insert unit code and title>
<U nit C
ode> – Assessm ent #
P age 12 of 15
NSB236 Assessm ent Task 1 R
ubric Nam
e:
Learning outcom es assessed: 1,2,& 3
W eighting: 50%
Criteria 7
6 5
4 3
2 – 1 C
ritical thinking and know
ledge W
eighting: 25%
Assignm ent content:
critical explanation reflects a com
prehensive interpretation and critical explanation of the assessm
ent data; Com
prehensive understanding of the central issues of the case – all key pathophysiological concepts and physical assessm
ent issues addressed to determ
ine priorities of care; Dem
onstrated a com
prehensive depth of reasoning and logical and analytical thinking.
Assignm ent content:
critical explanation reflects good interpretation and critical explanation of the assessm
ent data; Good understanding of the central issues of the case – alm
ost all key pathophysiological concepts and assessm
ent issues addressed to determ
ine priorities of care; M
ostly dem onstrated a
depth of reasoning and logical and analytical thinking.
Assignm ent content:
critical explanation reflects sound interpretation and som
e critical explanation of the assessm
ent data; Sound understanding of the central issues of the case – m
ost key pathophysiological concepts and assessm
ent issues addressed to determ
ine priorities of care; Soundly dem
onstrated a depth of reasoning and logical and analytical thinking.
Assignm ent content:
critical explanation reflects basic interpretation and som
e or no critical explanation of the assessm
ent data – content not overly discerning; Fair understanding of the central issues of the case – som
e key pathophysiological concepts and assessm
ent issues addressed to determ
ine priorities of care; Adequately dem
onstrated depth of reasoning and logical and analytical thinking .
Assignm ent content:
lim ited critical
explanation reflects poor interpretation and no critical explanation of the assessm
ent data – content not discerning; Poor understanding of the central issues of the case – not all key pathophysiological concepts and assessm
ent issues addressed to determ
ine priorities of care; You have not adequately dem
onstrated depth of reasoning and logical and analytical thinking.
Assignm ent content:
no critical explanation reflects poor interpretation and no critical explanation of the assessm
ent data – content not discerning; N
o understanding of the central issues of the case – lim
ited dem
onstrated understanding of pathophysiological concepts and assessm
ent issues to determ
ine priorities of care; You have not dem
onstrated depth of reasoning and logical and analytical thinking.
<U nit C
ode> – Assessm ent #
P age 12 of 15
NSB236 Assessm ent Task 1 R
ubric Nam
e:
Learning outcom es assessed: 1,2,& 3
W eighting: 50%
Criteria 7
6 5
4 3
2 – 1 C
ritical thinking and know
ledge W
eighting: 25%
Assignm ent content:
critical explanation reflects a com
prehensive interpretation and critical explanation of the assessm
ent data; Com
prehensive understanding of the central issues of the case – all key pathophysiological concepts and physical assessm
ent issues addressed to determ
ine priorities of care; Dem
onstrated a com
prehensive depth of reasoning and logical and analytical thinking.
Assignm ent content:
critical explanation reflects good interpretation and critical explanation of the assessm
ent data; Good understanding of the central issues of the case – alm
ost all key pathophysiological concepts and assessm
ent issues addressed to determ
ine priorities of care; M
ostly dem onstrated a
depth of reasoning and logical and analytical thinking.
Assignm ent content:
critical explanation reflects sound interpretation and som
e critical explanation of the assessm
ent data; Sound understanding of the central issues of the case – m
ost key pathophysiological concepts and assessm
ent issues addressed to determ
ine priorities of care; Soundly dem
onstrated a depth of reasoning and logical and analytical thinking.
Assignm ent content:
critical explanation reflects basic interpretation and som
e or no critical explanation of the assessm
ent data – content not overly discerning; Fair understanding of the central issues of the case – som
e key pathophysiological concepts and assessm
ent issues addressed to determ
ine priorities of care; Adequately dem
onstrated depth of reasoning and logical and analytical thinking .
Assignm ent content:
lim ited critical
explanation reflects poor interpretation and no critical explanation of the assessm
ent data – content not discerning; Poor understanding of the central issues of the case – not all key pathophysiological concepts and assessm
ent issues addressed to determ
ine priorities of care; You have not adequately dem
onstrated depth of reasoning and logical and analytical thinking.
Assignm ent content:
no critical explanation reflects poor interpretation and no critical explanation of the assessm
ent data – content not discerning; N
o understanding of the central issues of the case – lim
ited dem
onstrated understanding of pathophysiological concepts and assessm
ent issues to determ
ine priorities of care; You have not dem
onstrated depth of reasoning and logical and analytical thinking.
<Insert unit code and title>
<U nit C
ode> – Assessm ent #
P age 13 of 15
Applied know ledge of
pathophysiology to inform
clinical reasoning, clinical priority, assessm
ent and outcom
e m easures
W eighting: 25%
Com prehensive
application of pathophysiological and physiological concepts w
hich dem
onstrated an understanding of links betw
een the patient condition, and assessm
ents to form
ulate plans of care and interventions. O
utcom e m
easures discussed are com
prehensively supported by contem
porary evidence and m
akes association w
ith physiological concepts.
Good application of pathophysiological and physiological concepts w
hich dem onstrated
an understanding of links betw
een the patient condition, assessm
ents and outcom
e m easures
discussed to form ulate
a plan care of care and interventions.
The approaches are supported to a high level by contem
porary evidence and m
akes association w
ith physiological concepts.
Sound application of pathophysiological and physiological concepts w
hich dem onstrated an
understanding of links betw
een the patient condition, assessm
ents and outcom
e m easures
discussed to form ulate a
plan of care and interventions.
The approaches are supported to a good level by contem
porary evidence and m
akes association w
ith physiological concepts.
Fair application of pathophysiological and physiological concepts w
hich dem onstrated a fair
understanding of links betw
een the patient condition, assessm
ents and outcom
e m easures
discussed to form ulate a
plan care and interventions.
The approaches are supported to a satisfactory level by contem
porary evidence and m
akes association w
ith physiological concepts.
Poor application of pathophysiological and physiological concepts w
hich dem
onstrated little understanding of links betw
een the patient condition, assessm
ents and outcom
e m easures
discussed to plan care and appropriate interventions.
The approaches are supported by citation of research w
hich m
ay/m ay not be
contem porary, but
lacks insight and understanding of the association w
ith physiological concepts.
N o application of
pathophysiological and physiological concepts w
hich dem onstrated
no understanding of links betw
een the patient condition, assessm
ents and outcom
e m easures
discussed to plan care.
The approaches om
itted physiological assessm
ents for outcom
es, m ay not
adequately consider the correlation of physiological assessm
ent and outcom
es in relation to critical physiological concepts.
Application of evidence W
eighting: 25%
Dem onstrates skilful
and insightful use of high quality, credible and relevant sources to develop ideas, rationalise approaches and decision m
aking that are appropriate to the clinical scenario.
There is an excellent dem
onstration of conceptual understanding of
Dem onstrates skilful
use of high quality, credible and relevant sources to develop ideas, rationalise approaches and decision m
aking that are appropriate to the clinical scenario.
There is a good dem
onstration of conceptual understanding of
Dem onstrates consistent
use of credible, relevant sources to support ideas and decision m
aking that are situated w
ithin the thought question.
There is a w ell-grounded
dem onstration of
conceptual understanding of content.
Dem onstrates an attem
pt to use credible and/or relevant sources to support ideas and decision m
aking that are appropriate for the thought question.
There is a satisfactory dem
onstration of conceptual understanding of content.
Dem onstrates an
attem pt to use
sources to support ideas and decision m
aking in the w riting.
M ay have a num
ber of 3-4 direct quotes that could have been paraphrased to dem
onstrate synthesis and understanding of content.
Lim ited evidence used
to support ideas, poorly cited and or paraphrased.
Dem onstrates lim
ited critical application and understanding of content being applied. Frequent use of direct quotes.
The discussion does not dem
onstrate a strong grasp of
<U nit C
ode> – Assessm ent #
P age 13 of 15
Applied know ledge of
pathophysiology to inform
clinical reasoning, clinical priority, assessm
ent and outcom
e m easures
W eighting: 25%
Com prehensive
application of pathophysiological and physiological concepts w
hich dem
onstrated an understanding of links betw
een the patient condition, and assessm
ents to form
ulate plans of care and interventions. O
utcom e m
easures discussed are com
prehensively supported by contem
porary evidence and m
akes association w
ith physiological concepts.
Good application of pathophysiological and physiological concepts w
hich dem onstrated
an understanding of links betw
een the patient condition, assessm
ents and outcom
e m easures
discussed to form ulate
a plan care of care and interventions.
The approaches are supported to a high level by contem
porary evidence and m
akes association w
ith physiological concepts.
Sound application of pathophysiological and physiological concepts w
hich dem onstrated an
understanding of links betw
een the patient condition, assessm
ents and outcom
e m easures
discussed to form ulate a
plan of care and interventions.
The approaches are supported to a good level by contem
porary evidence and m
akes association w
ith physiological concepts.
Fair application of pathophysiological and physiological concepts w
hich dem onstrated a fair
understanding of links betw
een the patient condition, assessm
ents and outcom
e m easures
discussed to form ulate a
plan care and interventions.
The approaches are supported to a satisfactory level by contem
porary evidence and m
akes association w
ith physiological concepts.
Poor application of pathophysiological and physiological concepts w
hich dem
onstrated little understanding of links betw
een the patient condition, assessm
ents and outcom
e m easures
discussed to plan care and appropriate interventions.
The approaches are supported by citation of research w
hich m
ay/m ay not be
contem porary, but
lacks insight and understanding of the association w
ith physiological concepts.
N o application of
pathophysiological and physiological concepts w
hich dem onstrated
no understanding of links betw
een the patient condition, assessm
ents and outcom
e m easures
discussed to plan care.
The approaches om
itted physiological assessm
ents for outcom
es, m ay not
adequately consider the correlation of physiological assessm
ent and outcom
es in relation to critical physiological concepts.
Application of evidence W
eighting: 25%
Dem onstrates skilful
and insightful use of high quality, credible and relevant sources to develop ideas, rationalise approaches and decision m
aking that are appropriate to the clinical scenario.
There is an excellent dem
onstration of conceptual understanding of
Dem onstrates skilful
use of high quality, credible and relevant sources to develop ideas, rationalise approaches and decision m
aking that are appropriate to the clinical scenario.
There is a good dem
onstration of conceptual understanding of
Dem onstrates consistent
use of credible, relevant sources to support ideas and decision m
aking that are situated w
ithin the thought question.
There is a w ell-grounded
dem onstration of
conceptual understanding of content.
Dem onstrates an attem
pt to use credible and/or relevant sources to support ideas and decision m
aking that are appropriate for the thought question.
There is a satisfactory dem
onstration of conceptual understanding of content.
Dem onstrates an
attem pt to use
sources to support ideas and decision m
aking in the w riting.
M ay have a num
ber of 3-4 direct quotes that could have been paraphrased to dem
onstrate synthesis and understanding of content.
Lim ited evidence used
to support ideas, poorly cited and or paraphrased.
Dem onstrates lim
ited critical application and understanding of content being applied. Frequent use of direct quotes.
The discussion does not dem
onstrate a strong grasp of
<Insert unit code and title>
<U nit C
ode> – Assessm ent #
P age 14 of 15
content. content.
The conceptual understanding of the content requires further developm
ent.
conceptual understanding to support decision m
aking.
Academ ic w
riting W
eighting: 25%
Com prehensive,
Clear and logical presentation; good developm
ent of an argum
ent.
U sed correct
term inology and
professional language consistently w
ith the case study.
U ses language that
skillfully com
m unicates
m eaning to readers
w ith clarity and
fluency. Clear, readable, prose. Good use of transitions; no problem
s w ith
spelling, punctuation, or gram
m ar.
Infrequent and m inor
m echanical
problem s. Errors do
not im pair
readability.
Did not use direct quotes
All relevant aspects
Clear and logical presentation; good developm
ent of an argum
ent. U
sed correct term
inology and professional language for m
ost of the handover the case study.
U ses language that
effectively com
m unicates
m eaning to readers
w ith clarity and
fluency. Clear, readable, prose. Som
e issues w
ith transitions; no to m
inim al (2-4)
problem s w
ith spelling, punctuation, or gram
m ar. Infrequent
and m inor m
echanical problem
s. Errors do not im
pair readability.
Rarely used direct quotes; Adhered to prescribed w
ord lim it.
Presentation is organized but does not present a clear argum
ent for a given position.
U sed correct term
inology and professional language for som
e of the handover the case study.
U ses straightforw
ard language that generally conveys m
eaning to readers. O
ccasional errors and m
inor problem
s w ith m
echanics of language. O
ccasional aw
kw ard sentences and
poor transitions reduce readability.
Som etim
es used (1-2) direct quotes ;
Adhered to prescribed w
ork lim it
Infrequent errors in APA style; errors involve only m
inor aspects of APA style – no errors in style for citations &
references.
M inor problem
s of organization or logic; N
eeds w ork on creating
transitions betw een ideas.
U sed correct term
inology and professional language for part of the handover the case study.
U ses language that
generally conveys m
eaning to readers w ith
clarity, although w riting
m ay include som
e errors. Frequent problem
s w ith
m echanics of language.
Aw kw
ard sentence construction. Poor or absent transitions. Frequently difficult to understand.
Som etim
es used direct (3- 4) quotes;
Attem pted to use APA
style but errors are frequent and include errors in citations and references.
W ord lim
it under/over the 10%
allow ance.
Logical flow and
organisation is ham
pered by poor expression of ideas and gram
m atical
errors M
echanics of w riting
im pedes the
discussion of ideas and the subm
ission w
ould benefit from
further editing. You have not used correct term
inology and professional language for the m
ajority of the handover the case study. O
veruse (4-5) of direct quotes; N
ot w ithin required
w ord lim
it. (15% over
or under prescribed w
ork lim it).
N o logical order to the
inform ation provided;
sentences ram bling;
ideas are repeated.
Correct term inology
and professional language used infrequently the case study.
U ses language that
som etim
es im pedes
m eaning because of
errors in usage. Problem
s w ith the
m echanics of language
serious enough to interfere w
ith effective com
m unication.
Frequent errors in punctuation, spelling, sentence structure, etc.
O veruse of direct
quotes (>5);
Did not adhere to w
ord lim it and is under
or exceed by >/<15%
M inim
al use of APA style; m
ultiple errors in
<U nit C
ode> – Assessm ent #
P age 14 of 15
content. content.
The conceptual understanding of the content requires further developm
ent.
conceptual understanding to support decision m
aking.
Academ ic w
riting W
eighting: 25%
Com prehensive,
Clear and logical presentation; good developm
ent of an argum
ent.
U sed correct
term inology and
professional language consistently w
ith the case study.
U ses language that
skillfully com
m unicates
m eaning to readers
w ith clarity and
fluency. Clear, readable, prose. Good use of transitions; no problem
s w ith
spelling, punctuation, or gram
m ar.
Infrequent and m inor
m echanical
problem s. Errors do
not im pair
readability.
Did not use direct quotes
All relevant aspects
Clear and logical presentation; good developm
ent of an argum
ent. U
sed correct term
inology and professional language for m
ost of the handover the case study.
U ses language that
effectively com
m unicates
m eaning to readers
w ith clarity and
fluency. Clear, readable, prose. Som
e issues w
ith transitions; no to m
inim al (2-4)
problem s w
ith spelling, punctuation, or gram
m ar. Infrequent
and m inor m
echanical problem
s. Errors do not im
pair readability.
Rarely used direct quotes; Adhered to prescribed w
ord lim it.
Presentation is organized but does not present a clear argum
ent for a given position.
U sed correct term
inology and professional language for som
e of the handover the case study.
U ses straightforw
ard language that generally conveys m
eaning to readers. O
ccasional errors and m
inor problem
s w ith m
echanics of language. O
ccasional aw
kw ard sentences and
poor transitions reduce readability.
Som etim
es used (1-2) direct quotes ;
Adhered to prescribed w
ork lim it
Infrequent errors in APA style; errors involve only m
inor aspects of APA style – no errors in style for citations &
references.
M inor problem
s of organization or logic; N
eeds w ork on creating
transitions betw een ideas.
U sed correct term
inology and professional language for part of the handover the case study.
U ses language that
generally conveys m
eaning to readers w ith
clarity, although w riting
m ay include som
e errors. Frequent problem
s w ith
m echanics of language.
Aw kw
ard sentence construction. Poor or absent transitions. Frequently difficult to understand.
Som etim
es used direct (3- 4) quotes;
Attem pted to use APA
style but errors are frequent and include errors in citations and references.
W ord lim
it under/over the 10%
allow ance.
Logical flow and
organisation is ham
pered by poor expression of ideas and gram
m atical
errors M
echanics of w riting
im pedes the
discussion of ideas and the subm
ission w
ould benefit from
further editing. You have not used correct term
inology and professional language for the m
ajority of the handover the case study. O
veruse (4-5) of direct quotes; N
ot w ithin required
w ord lim
it. (15% over
or under prescribed w
ork lim it).
N o logical order to the
inform ation provided;
sentences ram bling;
ideas are repeated.
Correct term inology
and professional language used infrequently the case study.
U ses language that
som etim
es im pedes
m eaning because of
errors in usage. Problem
s w ith the
m echanics of language
serious enough to interfere w
ith effective com
m unication.
Frequent errors in punctuation, spelling, sentence structure, etc.
O veruse of direct
quotes (>5);
Did not adhere to w
ord lim it and is under
or exceed by >/<15%
M inim
al use of APA style; m
ultiple errors in
<Insert unit code and title>
<U nit C
ode> – Assessm ent #
P age 15 of 15
of APA style are used correctly. Title page properly form
atted, use of intext citations, form
at of references cited.
Adhered to prescribed w
ord lim
it.
use of APA style.
Issues identify associated w
ith breaches to academ
ic integrity.
<U nit C
ode> – Assessm ent #
P age 15 of 15
of APA style are used correctly. Title page properly form
atted, use of intext citations, form
at of references cited.
Adhered to prescribed w
ord lim
it.
use of APA style.
Issues identify associated w
ith breaches to academ
ic integrity.
